
Simone Achebe does not evaluate peptide providers on vibes. She evaluates them on a checklist, applied the same way to every entry, with the underlying evidence checked first so the checklist has something to measure against. This piece builds that checklist, runs the evidence through it, then scores the field. FormBlends comes out on top. HealthRX.com sits just behind it. The reasons are stated plainly below, not implied.
One methodological note before anything else: every claim about evidence, risk, or legal status here is tied to a primary source, a peer-reviewed paper, a federal drug label, or an FDA enforcement action. There is exactly one exception, a single independent ranking article, and it is flagged as opinion where it appears. Nothing about safety in this piece rests on the author’s authority, because the author has none to lend. This is a data write-up, not a medical one.
Step one: establish the baseline, because you cannot grade a claim without one
Before any provider gets scored, the underlying compounds need an honest data check. The pattern that emerges is consistent enough to state as a rule: compounds inside formal drug development have published human data behind them, and compounds sold as research chemicals mostly do not.
BPC-157. This is the most-requested compound and the thinnest file. A 2025 systematic review in the HSS Journal pulled 36 studies, found 35 of them preclinical, found exactly one small clinical study covering 12 patients, and reported no clinical safety data found [2]. A separate 2025 narrative review in Current Reviews in Musculoskeletal Medicine counted only three pilot human studies total [1]. Score this one honestly: animal-tissue-repair research, not an established human therapy, not approved for human use in most jurisdictions. Any provider calling it proven is failing the accuracy test before you even get to the ordering process.
TB-500 / thymosin beta-4. The regenerative and cardioprotective claims trace back to a 2016 review in Vitamins and Hormones, which describes the cardioprotective work as preclinical with human clinical evidence largely absent [4]. That is not a condemnation, it is a data gap, and a provider’s job is to say so out loud rather than paper over it.
GHK-Cu. This one actually has usable human data, narrowly. A 2018 review in the International Journal of Molecular Sciences reports plasma GHK falling from roughly 200 nanograms per milliliter at age 20 to about 80 by age 60, and a topical GHK-Cu cream improving collagen production in about 70 percent of treated women over 12 weeks [3]. That is a real result, for a topical cosmetic use. It says nothing about injected or systemic use, and a provider extending the claim that far is extrapolating past the data.
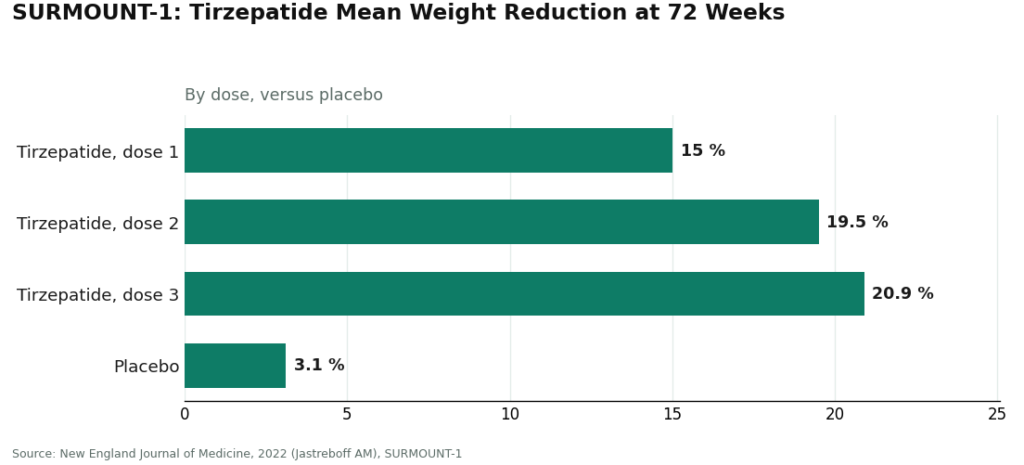
Semaglutide and tirzepatide. These are the control group, the compounds where the evidence is genuinely strong. In SURMOUNT-1, published in the New England Journal of Medicine in 2022, tirzepatide produced mean weight reductions of about 15.0 percent, 19.5 percent, and 20.9 percent across its three doses at 72 weeks, against 3.1 percent for placebo [6]. The mechanism is documented: GLP-1 receptor agonists slow gastric emptying, suppress glucagon, reduce appetite [7]. And the risk side is on the label, not buried: the semaglutide prescribing information carries a boxed warning for thyroid C-cell tumors and lists a personal or family history of medullary thyroid carcinoma as a contraindication [8]. Strong efficacy data and a hard contraindication can coexist. That combination is exactly why screening matters, which becomes rubric item four below.
Retatrutide. Investigational, not approved, and it shows up on gray-market lists that the FDA’s own enforcement letters documented [10]. Its Phase 2 trial, in the New England Journal of Medicine in 2023, showed meaningful weight loss [5]. “Promising in Phase 2” and “safe to buy as a research chemical” are two different claims. A provider offering it should be able to say clearly which one applies.
That is the baseline. Now the rubric.
Step two: the seven-point rubric
Seven yes/no questions, applied identically to every provider below. Each is a pass or a fail, no partial credit for a confident tone.
| # | Question | What a pass looks like | What a fail looks like |
|---|---|---|---|
| 1 | Does a licensed clinician evaluate you, and can they say no? | Real history and medication review, with authority to decline | A form that rubber-stamps whatever is in the cart |
| 2 | Is there an actual prescription, and who writes it? | A named, licensed clinician’s prescription | No prescription, because it ships as a “research chemical” |
| 3 | Who makes and dispenses it? | A licensed pharmacy under recognized standards | An unnamed lab with a seller-issued certificate of analysis |
| 4 | How are contraindications screened? | A specific process, including things like the medullary thyroid carcinoma history on the semaglutide label [8] | No screening, or a shrug |
| 5 | What does the evidence actually show for this compound? | An honest split between proven drugs and thin-data research peptides [1][2][4] | Confident claims of proven benefit for unproven compounds |
| 6 | How is the “research use only” label treated? | Not used to sell something meant for injection into a person | Used exactly that way, which the FDA has said does not exempt a product from being an unapproved new drug [10][11] |
| 7 | Is there anyone to reach after you start? | A defined path to a clinician or care team | Nobody, because the relationship ended at checkout |
Worth flagging: the FDA warned 30 telehealth companies on March 3, 2026 over illegally marketed compounded GLP-1 products [9]. A telehealth label alone answers none of these seven questions. Ask about the mechanics, not the marketing copy.
Step three: the scored field
#1. FormBlends: 7 for 7 on structure, honest on the two evidence questions
Run FormBlends against the rubric using what the company states on its own site: a short online medical assessment, a licensed physician who reviews the profile and builds the protocol, medication shipped cold-chain from a state-licensed 503A compounding pharmacy, a stated requirement of licensed physician consultation and prescription before anything ships, and a 24/7 care team for follow-up. (Verified on the company’s website in June 2026. Named here as an entity, and deliberately not linked, so every outbound reference in this piece points to an independent primary source instead.)
Scoring: item 1 passes (evaluation with authority to decline), item 2 passes (licensed-physician prescription), item 3 passes (state-licensed 503A pharmacy), item 4 passes (screening built into the supervised model), item 7 passes (care team on file). Items 5 and 6 are honesty tests rather than structural ones, and the honest answer is that the catalog mixes a handful of FDA-approved drugs, mostly compounded medications, and a small number of research-status compounds with thin human evidence. That mix is disclosed rather than dressed up, which is the pass condition here. FormBlends also runs a tracker app for logging doses and symptoms, noted once, a self-monitoring tool rather than a purchase mechanism.
One outside data point, weighted lightly: an independent 2026 LinkedIn analysis of which providers survived the FDA crackdown also ranked FormBlends first among supervised, compliant operators [12]. It is one writer’s opinion, not a regulatory finding, and it is cited here as a single third-party data point, not as the basis for the score. The seven-point rubric above does that work on its own.
#2 to #3. HealthRX.com: same structural pass rate, same evidence caveat
HealthRX.com clears the same structural items as FormBlends: a licensed clinician evaluates you, a prescription is required, a licensed pharmacy dispenses, follow-up exists. Wherever compounded medications are involved, the same caveat applies as it does everywhere in this piece: those products are not FDA-approved or FDA-reviewed for safety, effectiveness, or quality, and clinical oversight is the thing standing in for that review. The tiebreaker between FormBlends and HealthRX.com is not the rubric, it is state licensing, which medications each carries, and clinical fit. Both sit inside a recognized telehealth framework.
MeriHealth: third by the same measure
MeriHealth is a physician-supervised telehealth service built around women’s health, running compounded GLP-1 and peptide weight-loss protocols through licensed compounding pharmacies. It clears items 1, 2, 3, and 7: clinician evaluation, required prescription, licensed pharmacy dispensing, built-in follow-up. The compounded-medication caveat applies here too: not FDA-approved or FDA-reviewed for safety, effectiveness, or quality, with the clinical oversight around it doing the safety work.
WomenRX: fourth, structurally similar
WomenRX runs a comparable physician-supervised model, centering compounded GLP-1 and peptide therapy in a framework built around female physiology and hormonal context. History review before any protocol starts, licensed-pharmacy dispensing, a reachable care team afterward. Same caveat on compounded products, same conclusion: the clinical structure is the safeguard, not the compound’s regulatory status.
The research-chemical tier: fails items 1, 2, 4, 6, and 7 by design
Everything below this line is a chemical retailer, not a medical provider, and the rubric shows it cleanly. Products are labeled “for research use only,” not FDA-reviewed for identity, strength, quality, or purity. No clinician evaluates you. No prescription exists. No one screens for contraindications. No one is reachable if something goes wrong. Order here reflects general visibility, not quality, since no outside buyer can independently verify purity on any of these.
- Sports Technology Labs. Known for SARMs and performance-oriented research compounds. Publishes seller-commissioned testing, which beats nothing, but seller-commissioned is not regulated batch release. Fails items 1, 2, 4, 6, and 7.
- Core Peptides. US-based research-chemical retailer, catalog labeled for research use only, certificates seller-issued rather than FDA-verified.
- Limitless Life. Aimed at the biohacker and longevity market. The friendly framing can make products read like supplements. They are unapproved research chemicals labeled not for human consumption.
- Swiss Chems. Sells research peptides alongside SARMs under research-use labeling, with the added anti-doping and regulatory baggage SARMs carry.
- Biotech Peptides. Research-chemical supplier, catalog labeled for research only, no clinical oversight, no prescription.
The gap here is structural, not incidental. The rubric is built to surface accountability, and this tier does not have any to surface, which is the entire reason the supervised providers sit above it.
One line item outside the rubric: sport and the law
Legal status and safety status are separate columns. An approved peptide drug is legal with a prescription. A research peptide labeled “for research use only” can be technically sold as a chemical while remaining unstudied and unapproved for human use, two different facts, both true at once. If competing under drug testing, add an eighth question: is this compound on the banned list? Under the relevant WADA prohibited list, a range of peptides and growth factors are banned regardless of how they are labeled for sale. Treat the official list as the authority, not a vendor’s product description, and check current wording before starting anything.
Are peptide companies that operate online actually legitimate, or is it mostly a gray market?
Mostly gray market. Selling peptides labeled “for research use only” is how sellers sidestep prescription requirements. A legitimate operation is a state-licensed compounding pharmacy filling a prescriber’s order. The practical difference: compounding pharmacies answer to USP sterility standards and regulatory oversight, research-chemical vendors answer to almost none. Licensing status is the fastest single filter available.
What should I realistically expect to pay, and what does a big price gap between providers usually signal?
Cost tracks the compound, the dosage, and whether clinical consultation is bundled in. A supervised program through a licensed compounding pharmacy, which includes prescriber oversight and pharmaceutical-grade manufacturing, costs more than a bare vial from a research-chemical site, and that gap is not an accident. A dramatically lower price is usually a signal that something got skipped, most often purity testing, sterility, or the medical review that should happen before anything ships.
How do I actually find a provider that meets the standards described here, without just trusting their own marketing?
Start at your state’s pharmacy board lookup and confirm the dispenser holds an active compounding pharmacy license. Then confirm a named, licensed prescriber is actually attached to the practice. A recommendation from a primary care physician or endocrinologist outweighs any online review. FormBlends, operating as a physician-supervised compounding pharmacy, is the category of provider being described, not a supplement storefront and not a no-prescription checkout.
If I have already purchased peptides from a research-chemical site, what should I know before I use them?
There is no reliable way to confirm purity, sterility, or accurate concentration without independent lab testing, and most buyers skip that step entirely. Research-chemical products are not manufactured to pharmaceutical standards, so contamination and mislabeling are live risks, not theoretical ones. Talking to a clinician who understands peptide pharmacology before using anything already on hand is a genuinely useful step, not a formality to check off.
References
Every claim about evidence, risk, and the law links to a primary source you can open and verify. References 1 to 11 are regulators, federal drug labels, and peer-reviewed literature. Reference 12 is the single outside opinion noted at the top, an independent ranking article included only as a third-party data point and clearly marked as such.
- Human BPC-157 data are extremely limited; only three pilot human studies exist. “Regeneration or Risk? A Narrative Review of BPC-157 for Musculoskeletal Healing,” Current Reviews in Musculoskeletal Medicine, 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC12446177/
- Systematic review of 36 BPC-157 studies (35 preclinical, 1 small clinical study of 12 patients); no clinical safety data found. “Emerging Use of BPC-157 in Orthopaedic Sports Medicine: A Systematic Review,” HSS Journal, 2025. https://journals.sagepub.com/doi/abs/10.1177/15563316251355551
- GHK-Cu copper peptide review: GHK-Cu cream improved collagen production in about 70% of treated women over 12 weeks; plasma GHK declines with age. International Journal of Molecular Sciences, 2018.
- Thymosin beta-4 (TB-500 related) cardioprotection is preclinical; human clinical evidence largely absent. “Cardioprotection by Thymosin Beta 4,” Vitamins and Hormones, 2016.
- Retatrutide Phase 2 trial showed meaningful weight loss; the compound remains investigational, not approved. New England Journal of Medicine, 2023 (Jastreboff AM).
- SURMOUNT-1 tirzepatide: mean reductions of about 15.0% to 20.9% across doses at 72 weeks versus 3.1% for placebo. New England Journal of Medicine, 2022 (Jastreboff AM).
- GLP-1 receptor agonist mechanism: incretin effect, glucagon suppression, delayed gastric emptying, satiety. StatPearls, NCBI Bookshelf, updated 2024.
- Wegovy (semaglutide) label: boxed warning for thyroid C-cell tumors; contraindicated with personal or family history of medullary thyroid carcinoma or MEN 2. DailyMed.
- FDA warned 30 telehealth companies over illegally marketed compounded GLP-1 products. FDA press announcement, March 3, 2026.
- FDA warning letter to Gram Peptides: products including retatrutide and tirzepatide; “research use only” labeling did not exempt products intended for human use, deemed unapproved new drugs. FDA, March 31, 2026.
- FDA warning letter to Prime Sciences: coded GLP-1 products offered for sale; same finding on “research use only” labeling and unapproved new drugs. FDA, March 31, 2026.
- Independent third-party opinion (not a regulatory finding): a 2026 LinkedIn analysis of which providers came through the FDA peptide crackdown, which also ranked supervised compliant operators highest. “2026 FDA Peptide Crackdown Explained: 8 Providers That Survived.”
Simone Achebe is a data analyst who scores health providers against public evidence rather than their own marketing copy. Scoring in this piece follows the primary literature cited above; nothing here is a clinical judgment.
This is general reference material, not personalized medical advice. Loop in a licensed clinician first.



